Article Text

Abstract
Background: The reported prevalence of exercise induced asthma (EIA) in elite winter athletes ranges from 9% to 50%. Many elite winter athletes do not report symptoms of EIA. At present there is no gold standard test for EIA.
Objective: To establish the efficacy of screening for EIA and examine the role of the eucapnic voluntary hyperventilation (EVH) challenge and laboratory based and sport specific exercise challenges in the evaluation of elite winter athletes.
Methods: 14 athletes (mean (SD) age 22.6 (5.7) years, height 177.2 (7.0) cm, body mass 68.9 (16.9) kg) from the Great Britain short-track speed skating (n = 10) and biathlon teams (n = 4) were studied. Each athlete completed a laboratory based and sport specific exercise challenge as well as an EVH challenge, in randomised order.
Results: All 14 athletes completed each challenge. Two had a previous history of asthma. Ten (including the two with a previous history) had a positive test to at least one of the challenges. Ten athletes had a positive response to EVH; of these, only three also had a positive response to the sport specific challenge. No athletes had a positive response to the laboratory based challenge.
Conclusions: Elite athletes should be screened for EIA. EVH is a more sensitive challenge in asymptomatic athletes than sport specific and laboratory based challenges. If sporting governing bodies were to implement screening programmes to test athletes for EIA, EVH is the challenge of choice.
- EIA, exercise induced asthma
- EVH, eucapnic voluntary hyperventilation
- FEF50, forced expiratory flow at 50% of forced vital capacity
- FEV1, forced expiratory volume in one second
- FEV1%, FEV1 as a percentage of forced vital capacity
- FVC, forced vital capacity
- IOC-MC, International Olympic Committee-Medical Commission
- PEF, peak expiratory flow
- exercise induced asthma
- β2 agonist
- eucapnic voluntary hyperventilation
- exercise challenge
Statistics from Altmetric.com
- EIA, exercise induced asthma
- EVH, eucapnic voluntary hyperventilation
- FEF50, forced expiratory flow at 50% of forced vital capacity
- FEV1, forced expiratory volume in one second
- FEV1%, FEV1 as a percentage of forced vital capacity
- FVC, forced vital capacity
- IOC-MC, International Olympic Committee-Medical Commission
- PEF, peak expiratory flow
Exercise induced asthma (EIA) is defined as a transient narrowing of the airways, limiting expiration, following a bout of exercise, which is reversible by inhalation of β2 agonists.1 The reported prevalence of EIA in winter athletes ranges from 9% to 50%,2 which is higher than that of the general population (approximately 8% in the United Kingdom), but in line with estimates for elite summer sports athletes.3
At both the 2002 Salt Lake City Winter Olympics and the 2004 Athens Summer Olympics, athletes who wished to use inhaled β2 agonists therapeutically were required to provide evidence of asthma through bronchodilator or bronchial provocation challenges. At present, there is no gold standard test for EIA; however, the International Olympic Committee-Medical Commission (IOC-MC) accepts the results of various different airway challenges, including exercise, eucapnic voluntary hyperventilation (EVH), methacholine, and saline challenges.4
Exercise is an indirect airway challenge that has a high level of specificity,4 but its sensitivity is affected by environmental conditions.5 Accordingly, exercise challenges in sport specific environments are more sensitive than challenges conducted in laboratory settings.5 This is probably because the air conditioned laboratory environment has a relatively high temperature (around 20°C) and water content (around 50% relative humidity). Airway drying6,7,8,9,10 and airway cooling7,11,12 have been proposed as mechanisms in the aetiology of EIA. Therefore an air conditioned laboratory based environment may not be sufficiently provocative, especially for winter athletes, who train and compete at sub-zero temperatures, where the water content of the air is very low. Despite this, laboratory based exercise challenges are still used to test elite athletes for EIA.
Eucapnic voluntary hyperventilation (EVH) is a laboratory based indirect airway challenge that enables minute ventilation and environmental conditions to be controlled. The EVH challenge has been reported to be the most suitable method for diagnosing EIA in cold weather athletes.13,14 However, over half the requests for therapeutic use exemption for β2 agonists submitted for the 2002 Salt Lake City Winter Olympics employed direct airway challenges to establish EIA (that is, methacholine and histamine).4 The sensitivity and specificity of these methods have been challenged. Holzer et al10 screened 50 athletes for EIA using methacholine and EVH challenges and found that only nine athletes (18%) had a positive challenge to methacholine, whereas 25 (50%, including the nine methacholine positive athletes) had a positive EVH challenge. The investigators concluded that an EVH challenge was more sensitive and specific than a methacholine challenge for the diagnosis of EIA in athletes. Thus evidence suggests that direct airway challenges are not sufficiently sensitive or specific for use in athletes.
Owing to the lack of sensitivity and specificity of symptom based diagnosis15 and direct airway challenges,10 several groups have recently suggested that athletes should be screened for EIA using either EVH challenge or exercise challenges.3,16–21 Our aim in this study was to establish the efficacy of screening for EIA and examine the role of the EVH challenge and laboratory based and sport specific exercise challenges in the evaluation of elite winter athletes.
METHODS
Following ethical approval from Harrow local research ethics committee, 14 athletes (mean (SD) age 22.6 (5.7) years, height 177.2 (7.0) cm, weight 68.9 (16.9) kg) from the Great Britain short-track speed skating (n = 10) and biathlon teams (n = 4) volunteered to participate, providing written informed consent.
Each athlete completed a laboratory based challenge, a sport specific challenge, and a eucapnic voluntary hyperventilation challenge (EVH) in random order. If an athlete was using asthma medication they were instructed to stop the drug before each test (inhaled corticosteroids, three days before; inhaled long acting β2 agonist, two days before; inhaled short acting β2 agonist, on the day of the test).
Laboratory based exercise challenge
The laboratory based challenge required the athlete to run continuously on a treadmill for eight minutes (temperature 18°C, relative humidity (RH) 56%). Exercise intensity was set to elicit a heart rate of more than 90% of maximum (HRmax) for the final four minutes of exercise.22
Sport specific exercise challenge
The sport specific challenge for the speed skaters involved skating for six minutes (pace ranging between 11 and 12 seconds per 250 m lap) on the ice rink (temperature 8°C, RH 35%). The sport specific challenge for the biathletes involved a 20 minute simulated race in Vaukati, Finland (temperature 1–2°C, RH 31–34%).
Eucapnic voluntary hyperventilation
The EVH challenge was conducted in the laboratory and required each athlete to hyperventilate for six minutes (30× baseline forced expiratory volume in one second (FEV1)), breathing a gas mixture containing 5% CO2, 21% O2, and 74% N2 (inspired air temperature 19.1°C, RH >2%).23
A MicroLab ML3500 spirometer (Micro Medical, Rochester, Kent, UK) was used to collect all spirometry measurements. Maximum effort voluntary flow–volume loops were measured before and at 3, 5, 10, and 15 minutes after stopping each challenge. FEV1, peak expiratory flow (PEF), forced vital capacity (FVC), forced expiratory flow at 50% of FVC (FEF50), and FEV1 as a percentage of FVC (FEV1%) were recorded at each time point.
The percentage change (Δ) in FEV1, PEF, FVC, FEF50, and FEV1% were calculated for each challenge by taking the lowest value recorded in the 15 minutes following each challenge and expressing the difference between this and the baseline value measured immediately before each challenge as a percentage. A fall in FEV1 of 10% or more from the baseline value was deemed positive for EIA.
Statistical analysis
Repeated measure analysis of variance (ANOVA) tests were used to compare the changes in ΔFEV1, ΔPEF, ΔFVC, ΔFEF50, and ΔFEV1% for each challenge. Planned unpaired t tests were used to analyse the difference between positive and negative athletes for each challenge. A probability (p) value of <0.05 was regarded as significant. All values are presented as mean (SD).
RESULTS
All 14 athletes completed every challenge. Of the 14 athletes, two had a previous history of asthma and were currently treated with beclomethasone and salbutamol inhalers. Baseline lung function and ΔFEV1 for each challenge are reported for every athlete in table 1.
Athlete responses to each challenge
Based on a ⩾10% fall in FEV1, 10 of the 14 athletes (including two athletes with a previous history of asthma) had a positive response to at least one of the challenges (table 1). There was no significant difference between baseline FEV1 predicted values between athletes with positive EIA (102.9 (11.43)%) and negative EIA (110.25 (12.61)%). Ten athletes had a positive response to EVH; of these, only three also had a positive response to the sport specific challenge. No athletes had a positive test to the laboratory based challenge (figs 1–3).

Changes in forced expiratory volume in one second (ΔFEV1) for each athlete during laboratory based challenge (LB) compared with eucapnic voluntary hyperventilation (EVH). The 7% cut off criterion has been added to show the number of additional athletes who might have received a diagnosis of exercise induced asthma had this criterion been used for exercise challenges.
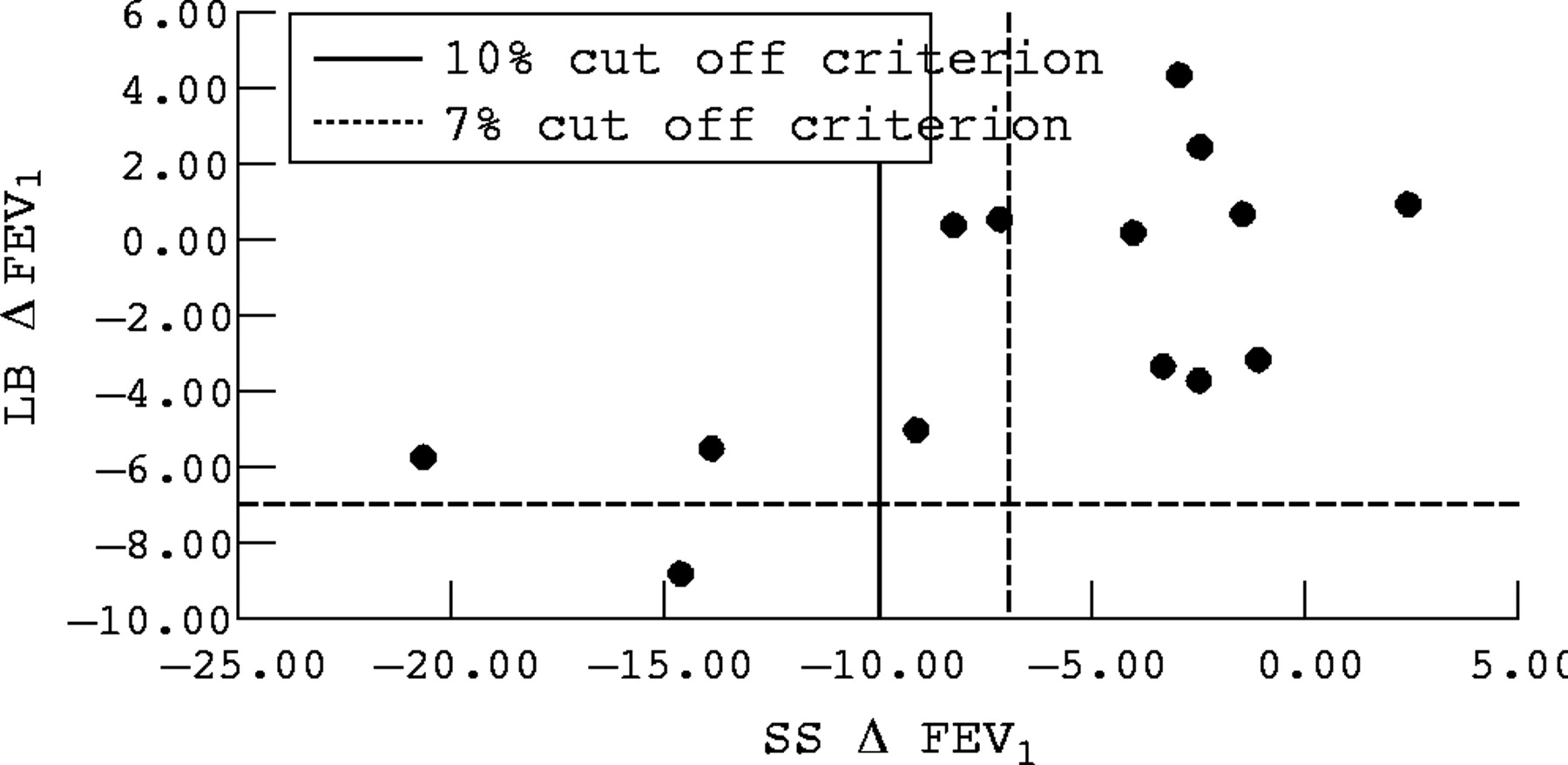
Changes in forced expiratory volume in one second (ΔFEV1) for each athlete during sport specific challenge (SS) compared with laboratory based challenge (LB). The 7% cut off criterion has been added to show the number of additional athletes who might have received a diagnosis of exercise induced asthma had this criterion been used for exercise challenges.
{kind=link}
{kind=link}
{kind=link}
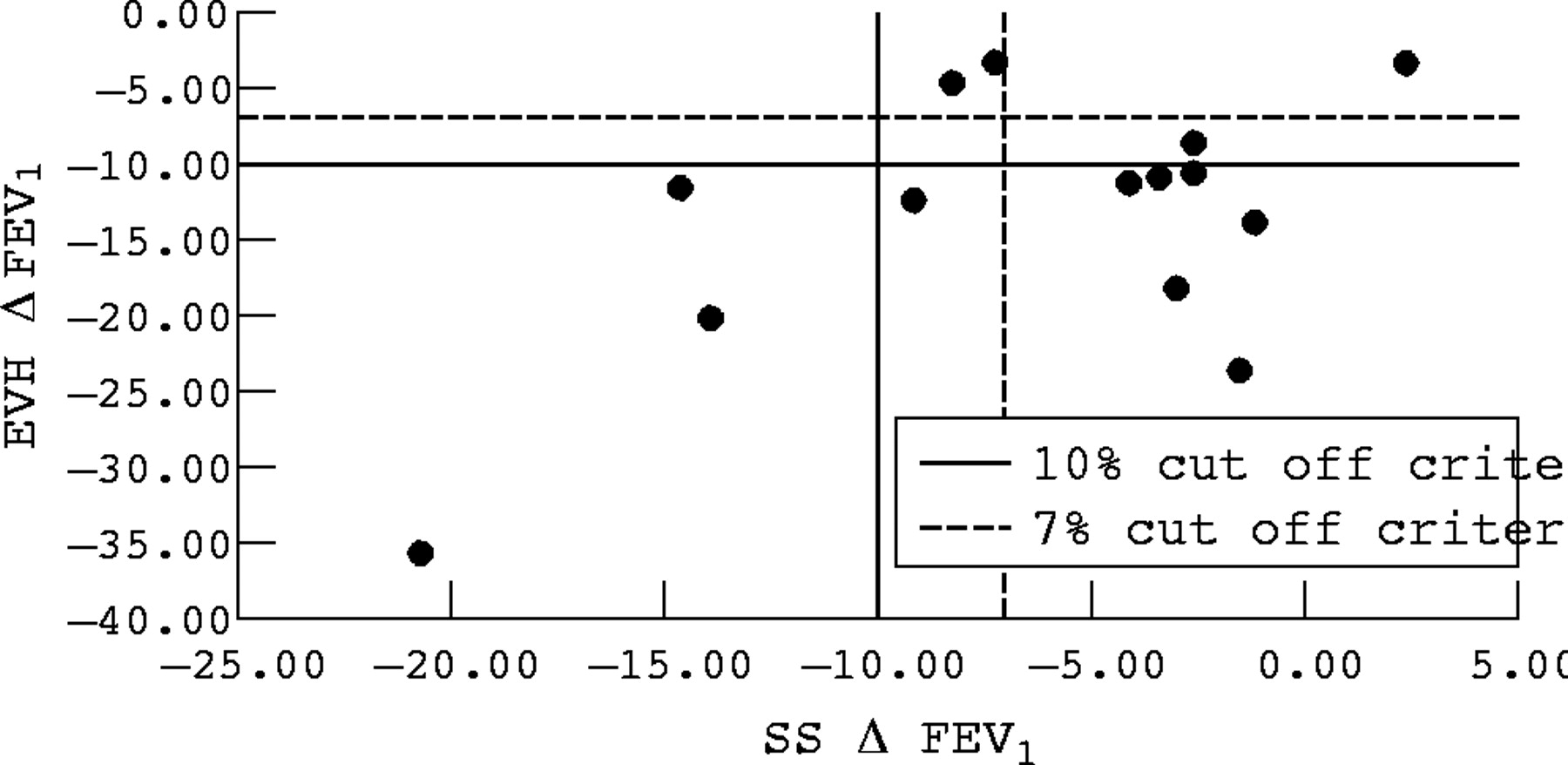
Changes in forced expiratory volume in one second (ΔFEV1) for each athlete during sport specific challenge (SS) compared with eucapnic voluntary hyperventilation (EVH). The 7% cut off criterion has been added to show the number of additional athletes who might have received a diagnosis of exercise induced asthma had this criterion been used for exercise challenges.
After the assumption of sphericity was met, repeated measures ANOVA showed that ΔFEV1, ΔPEF, ΔFEF50, and ΔFEV1% changes were significantly greater (p<0.05) following EVH than either the laboratory based or sport specific challenge. The average reductions for EIA positive (ΔFEV1 ⩾10% for at least one challenge) and EIA negative athletes following laboratory based, sport specific, and EVH challenges are reported in table 2.
Comparison of mean percentage changes for EIA positive and EIA negative athletes for the eucapnic voluntary hyperventilation and sport specific challenges
DISCUSSION
Our study suggests that screening elite athletes for EIA appears warranted. In addition to the two athletes who had a previous history of EIA, screening elite athletes resulted in the identification of eight others with no history of EIA who had significant bronchial hyperresponsiveness (>10% fall in FEV1). We have therefore highlighted the findings from previous studies that suggest that many athletes fail to report or to recognise symptoms of EIA.3,15–17
Our study showed that the EVH challenge resulted in a greater number of athletes presenting with bronchial hyperresponsiveness commensurate with a diagnosis of EIA than either a sport specific or a laboratory based exercise challenge. Our results are similar to studies that have compared exercise and EVH challenges13,14 and suggest that the EVH challenge provides a more sensitive diagnosis of EIA in elite winter athletes than the other routinely used non-pharmacological challenges. In our study all athletes who presented with EIA did so through the EVH challenge. In contrast, Rundell et al,14 studying 19 winter athletes with EIA, found that two had a positive exercise challenge but did not have a positive response to EVH. Had our study recruited a larger number of athletes we might have found that EVH did not identify all athletes with EIA. Nevertheless it is clear that EVH is a sensitive and specific challenge for EIA in elite athletes.
The superiority of the EVH challenge results primarily from the greater degree of control over the two main contributors to the airway response—the inspired air water content and minute ventilation. The enhanced control over the condition of the inhaled air and breathing rate during the EVH challenge allows greater confidence that the airways are being adequately stimulated to trigger bronchoconstriction in susceptible subjects.
In line with the greater control of inspired air water content during the EVH challenge, findings from the present study are consistent with the hyperosmolarity theory6,7,8,9,10 rather than the airway rewarming theory7,11,12 of EIA development. Despite the colder inspired air temperature during the sport specific challenge (1°C biathlon, 8°C speed skating) compared with the laboratory based challenge (18°C), only a three athletes had a positive response. The EVH challenge, which had the largest number of positive tests (10 athletes), was conducted with inspired air temperatures (19.1°C) similar to those of the laboratory based challenge; however, the relative humidity of the inspired air (<2%) was much lower than either the laboratory based (∼60%) or the sport specific challenge (31–35%). The provocative nature of dry air inhalation, rather than cold air, lends support to the notion that the underlying mechanisms EIA are not temperature related.
The smaller number of athletes who presented with EIA following sport specific and laboratory based challenges may be because the required 10% fall in FEV1 is not sensitive enough to detect EIA following laboratory based or sport specific challenges. Work by Helenius et al18,24 has suggested that the 10% cut off criterion for FEV1 may be insufficiently sensitive to detect EIA in elite athletes and it is not statistically justified. They suggested a fall in FEV1 of 6.5% as a suitable cut off criterion for elite runners, while Rundell et al5 suggested 7.1%. These values were based on the 95th centile (defined as two standard deviations) of the post-exercise decline in FEV1 observed in a non-asthmatic population.
In line with Rundell et al,5 a reduction in the cut off criterion to ΔFEV1 of 7% in the present study resulted in a further two athletes being classified as positive in the sport specific challenge, and four in the laboratory based challenge (figs 1 and 2). No false negative responses were observed. Further work is required to establish standardised cut off criteria for the decline in FEV1 following various challenges. This may show that the criterion for exercise challenges should be lower than that for an EVH challenge (FEV1 ⩾−10%).
In conclusion, our observations support the role of screening elite athletes for EIA and suggest that EVH is a more sensitive challenge for the detection of EIA in asymptomatic athletes than either sport specific or laboratory based challenges. Thus if sporting governing bodies were to implement screening programmes to test athletes for EIA our recommendation is that EVH should be the challenge of choice.
Acknowledgments
We are grateful to the European Olympic Committee, UK Sport, British Olympic Medical Trust and Micro Medical Ltd. (www.micromedical.co.uk)
REFERENCES
Commentary
Although this work is not novel, it does confirm and support previous studies evaluating the efficacy of eucapnic voluntary hyperventilation (EVH) as a tool for identifying exercise induced asthma. Previous studies have made similar comparisons with similar results (that is, it is quite well established that a laboratory challenge at room temperature and 50% relative humidity is not an appropriate provocative challenge). The study design is clear and the results solid, although a larger number of subjects would strengthen the study power. An important point to consider is whether or not small falls in FEV1 (∼10%) are of functional significance (in other words, do these small falls affect competition outcomes?); nonetheless, the IOC has set the liberal cut off criterion of a 10% fall in FEV1. It is important to note that because of to the potency of EVH, only qualified laboratories with appropriate rescue plans in place should entertain its use.
Footnotes
-
Competing interests: none declared