Risks of general anaesthesia in people with obstructive sleep apnoea
BMJ 2004; 329 doi: https://doi.org/10.1136/bmj.329.7472.955 (Published 21 October 2004) Cite this as: BMJ 2004;329:955
- Cindy den Herder (c.denherder{at}slaz.nl), resident in ear, nose, and throat surgery1,
- Joachim Schmeck, specialist registrar in anaesthesiology and intensive care medicine3,
- Dick J K Appelboom, specialist registrar in anaesthesiology2,
- Nico de Vries, specialist registrar in ear, nose, and throat surgery1
- 1 Department of Otolaryngology/Head and Neck Surgery, St Lucas Andreas Hospital, Jan Tooropstraat 164, 1006 AE, Amsterdam, Netherlands
- 2 Department of Anaesthesiology, St Lucas Andreas Hospital
- 3 Department of Anaesthesiology and Operative Intensive Care Medicine, University Hospital Mannheim, University of Heidelberg Theodor-Kutzer-Ufer, D-68167, Mannheim, Germany
- Correspondence to: C den Herder
- Accepted 5 August 2004
Introduction
Sleep is an integral part of human existence and is now, more than ever, the subject of clinical and research interest. Why do we spend approximately one third of our lives asleep? Sleep probably has a recovery function, especially for the brain. Throughout rapid eye movement sleep, neuronal connections in the catecholamine system are created, and this activity is essential to maintain cognitive function.w1 During rapid eye movement sleep in particular, the body is at its most relaxed state, and a three dimensional collapse of muscle (musculus genioglossus and musculus geniohyoideus) and fatty tissue around the upper airway may cause obstruction.1 When a pre-existent narrowing and slackening of the upper airway is also present,2 apnoeas (complete cessation of breathing for 10 seconds or more) or hypopnoeas (> 50% diminishing of airflow or oxygen desaturations > 3% for 10 seconds or more) may result. The prevalence of obstructive sleep apnoea in middle age is 2% for women and 4% for men.3 In practice, obstructive sleep apnoea seems to be under-reported; obstructive sleep apnoea is undiagnosed in an estimated 80% of patients.4
Patients with obstructive sleep apnoea are particularly vulnerable during anaesthesia and sedation.5 w2 This is not only the case for operations or other invasive interventions aiming at alleviation of obstructive sleep apnoea through reduction of the obstructive upper airway; even after surgery not related to obstructive sleep apnoea, such as hip and knee operations, patients with obstructive sleep apnoea are at risk of developing respiratory and cardiopulmonary complications postoperatively. Serious complications include reintubations and cardiac events.6 Anaesthetic management must focus on and deal with the increased likelihood of morphological alterations of the upper airway leading to an increased rate of difficulties in securing and maintaining a patent airway.7
In this review we discuss the various anaesthetic aspects of obstructive sleep apnoea, including preoperative, perioperative, and postoperative points of special interest. We also cover the various management options.
Sources and selection criteria
To write this review, we consulted the Cochrane Library and did a thorough Medline search. We read the full text of relevant papers found by using the keywords “obstructive sleep apnoea,” “airway management,” and “general anaesthesia.”
Summary points
Patients with obstructive sleep apnoea are at high risk of developing complications when having surgery or other invasive interventions under general anaesthesia, whether or not the surgery is related to obstructive sleep apnoea
Surgeons of all specialties, and especially anaesthetists, should be aware that undiagnosed obstructive sleep apnoea is common
They should be alert to patients who are at risk of having obstructive sleep apnoea and be aware of the potential preoperative and postoperative complications in such patients
Management options include alternative methods of pain relief, use of nasal continuous airway pressure before and after surgery, and surveillance in an intensive care unit, especially after nasal surgery in which packs are used
An algorithm for management of difficult airways should be established
Preoperative aspects
Recognition of obstructive sleep apnoea
Anaesthetists are the key figures in the early recognition of undiagnosed obstructive sleep apnoea, because of their role in preoperative screening. Heavy and persistent snoring, sudden awakenings accompanied by choking, apnoeas as observed by the bed partner,8 and excessive sleepiness during daytime5 9 are characteristic symptoms of obstructive sleep apnoea. Obstructive sleep apnoea can also be associated with a wide variety of other symptoms (box 1) and signs (box 2), which unfortunately are not very specific. The Epworth sleepiness scale can be used to screen for obstructive sleep apnoea, but its specificity and sensitivity are also low. Ideally, full night polysomnography is used to determine if obstructive sleep apnoea is present. Obesity (body mass index > 30) and especially a large neck circumference (> 44 cm) have a positive correlation with severe obstructive sleep apnoea, because these conditions involve extensive soft tissue enlargements of the upper airway.w3 Other predisposing factors include increasing age,10 male sex,3 and use of alcohol.w4
Box 1: Symptoms associated with obstructive sleep apnoea
Adults
Heavy persistent snoring
Excessive daytime sleepiness
Apnoeas as observed by bed partner
Choking sensations while waking up
Gastro-oesophageal reflux
Reduced ability to concentrate
Memory loss
Personality changes
Mood swings
Night sweating
Nocturia
Dry mouth in the morning
Restless sleep
Morning headache
Impotence
Children
Snoring
Restless sleep
Sleepiness
Hyperactivity
Aggression and behavioural disturbance
Frequent colds or coughing
Odd sleeping positions
Box 2: Physical characteristics associated with obstructive sleep apnoea
Nasal obstruction (deviation of the septum or hypertrophic conchae inferiores)
Oedematous or long soft palate or uvula
Hypertrophic tongue tonsils
Narrow oropharynx (large tonsils, redundant pharyngeal arches)
Adiposity or large neck circumference
Retrognathia
Maxillary hypoplasia
The risk of developing perioperative complications is increased not only by the presence of obstructive sleep apnoea but also, not surprisingly, by comorbidity. Patients with obstructive sleep apnoea seem to have hypertension and cardiovascular diseases more often than do other patients.11 w5 Polycythaemia, initiated by a hypoxia driven production of erythropoietin by the kidneys, is common,w6 as are episodes of arterial oxygen desaturations (PaO2 < 80%) accompanied by cardiac arrhythmias.11
Assessment of risk that tracheal intubation may be difficult
Alterations in craniofacial morphology contributing to obstructive sleep apnoea—such as macroglossia, retrognathia, a narrow hypopharynx because of fat deposition in the lateral walls of the pharynx, or an anteriorly displaced larynx—also have an impact on anaesthetic management.12 w7 Although no strong relation between cephalometric variables and the incidence of obstructive sleep apnoea has been found, two anatomical landmarks have been shown to be important in patients with obstructive sleep apnoea: an inferiorly positioned hyoid (distance between chin and hyoid bone) and increased length of the soft palate.13 w8
Mallampati constructed a staging system to predict difficult tracheal intubation,14 and this system was modified by Friedman to enable estimation of the success rate of uvulopalatopharyngoplasty at the same time (fig 1). The position of the tongue is assessed in relation to that of the soft palate and, depending on the size of the tongue, four stages can be distinguished.w9 In general, oral intubation is hindered when patients are categorised as Mallampati stage 3 or 4,12 14 although Siyam et al failed to find a correlation of this preoperative staging system with more difficult intubation.w10 Liistro et al showed that a high Mallampati score together with nasal obstruction is a risk factor for obstructive sleep apnoea, because the airway at oropharyngeal level is reduced owing to a larger tongue.w6

Staging system of Mallampati to predict difficult tracheal intubation, as modified by Friedman (to predict the outcome of uvulopalatopharyngoplasty). The size of the tongue is assessed in relation to that of the soft palate, while the tongue rests in the floor of the mouth. Stage 1 (top left): complete visualisation of the uvula, tonsils, and arches. Stage 2 (top right): complete visualisation of the uvula; the tonsils and arches are partly invisible. Stage 3 (bottom left): only the soft and hard palate are visible; the uvula is hidden. Stage 4 (bottom right): only the hard palate is visible
{kind=link}
Any patient diagnosed as having obstructive sleep apnoea or in whom it is suspected on the basis of clinical signs (obesity, limited mouth opening, or a large tongue) should be treated as having a difficult airway until proved otherwise. Orotracheal intubation, especially in severely obese patients with obstructive sleep apnoea, may be extremely difficult, and postoperative airway obstruction due to swelling or bleeding should be anticipated. Of course, no staging system can prevent unexpected difficulties in tracheal intubation.
Perioperative aspects
Premedication
Preoperative sedation with benzodiazepines 45 minutes before the induction of general anaesthesia has anticonvulsive and muscle relaxing effects on the upper airway musculature, causing an appreciable reduction of the pharyngeal space. Consequently, a higher risk of preoperative phases of hypopnoea and consecutive hypoxia and hypercapnia arises after administration, and oxygen saturation needs to be monitored adequately.15 w12 An effective anxiolytic agent will reduce the dose of anaesthetic needed to induce general anaesthesia, which may otherwise lead to an increased likelihood of cardiovascular complications. If needed, oxygen can be given by an insufflation mask preoperatively, and application of nasal continuous positive airway pressure might be necessary postoperatively.w2
Intubation technique
The main goal in all patients is to avoid inadequate ventilation and oxygenation resulting in hypoxaemia or hypercapnia and any associated haemodynamic changes (such as tachycardia, arrhythmia, and hypertension) leading to increased morbidity and mortality. Death, brain injury, cardiopulmonary arrest, airway trauma, and damage to teeth are among the adverse events associated with difficult airway management. A difficult airway is defined as the clinical situation in which a conventionally trained anaesthetist experiences difficulties with ventilation of the upper airway by facemask, difficulty with tracheal intubation, or both. The purpose of the American Society of Anesthesiologists' guidelines is to reduce the likelihood of adverse outcomes by providing basic recommendations.w13 Components of the preoperative physical examination of the airway are shown in the table.
Components of preoperative physical examination of airway that may indicate difficult intubationw13
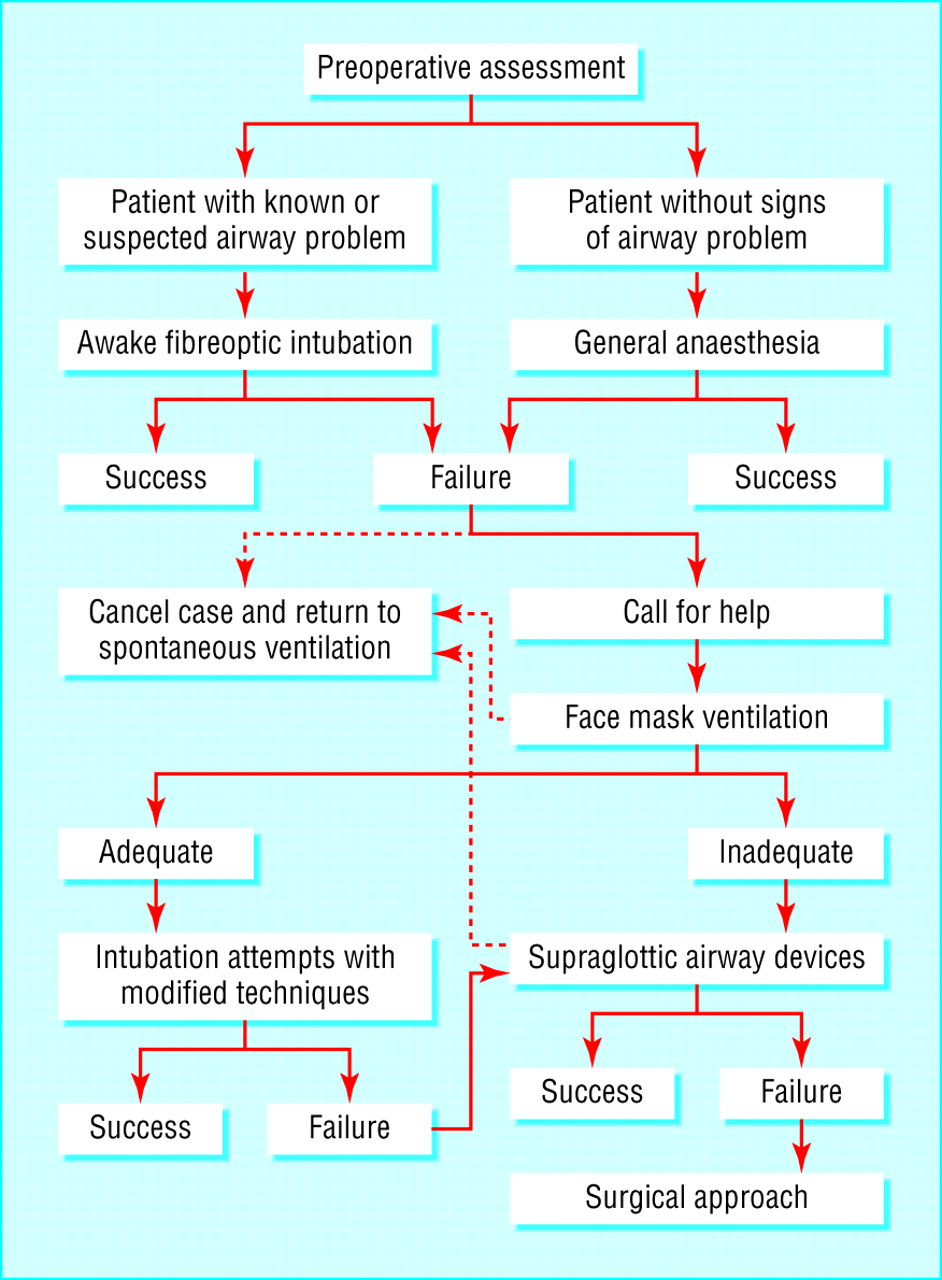
The equipment for management of a difficult airway should be in place before induction of general anaesthesia. Orotracheal tubes in various sizes, as well as a McCoy laryngoscope and a fastrach laryngeal mask, are necessary. Fibreoptic devices may be helpful but have no impact in acute emergency situations. A strategy or algorithm for establishing a secure airway should be defined (fig 2).

Algorithm for management of difficult airways
{kind=link}
Oxygen must be administered for three or more minutes before intubation and, whenever possible, during the process of establishing a secure airway and also after extubation. Endoscopically guided intubation with use of a “laryngeal airway mask” is an alternative, as is the use of a rigid ventilation-bronchoscope or an oesophageal-tracheal combitube. Patients with extreme anatomical anomalies should be intubated in alert condition with optimal local anaesthesia.w14 In the case of a ventilation emergency, surgical tracheostomy or needle cricothyrotomy should be considered early.16 Close cooperation with the ear, nose, and throat surgeon can be of value not only in these critical incidents but also in the preoperative and perioperative management of all patients with obstructive sleep apnoea.
Postoperative aspects
Extubating the difficult airway
The surgical procedure and the condition of the patient, as well as any documented or suspected trauma to the upper airway due to manipulations during the process of securing the airway, will influence the anaesthetist's strategy for extubating the patient with a difficult airway. Tracheal extubation should be carried out only when the patient is conscious, communicative, and breathing spontaneously with an adequate tidal volume and oxygenation. A half sitting or anti-Trendelenburg position is preferable.15 To avoid swelling of the pharynx after surgery, methylprednisolone is administered as a single bolus of 250 mg after the induction of general anaesthesia.17 Twenty minutes before the end of surgery, clonidine is infused (0.15 mg) to avoid extensive hypertension during the recovery phase and extubation, at the same time inducing a mild sedation without additional muscular relaxation. Most patients do not need continuous monitoring in the postoperative phase, but the decision to discharge these patients from the recovery room to a regular ward, an intermediate care unit, or an intensive care unit should be based on the type of procedure, the overall condition of the patient, and the infrastructure of the hospital.
Respiratory depression (arrest)
Respiratory depression and repetitive apnoeas often occur directly after extubation in patients with obstructive sleep apnoea.5 w2 Use of opioids increases this risk, and intravenous administration may cause delayed (4-12 hours after administration) respiratory depression.18 w15 w16 We believe that opioids should only be used when non-steroid anti-inflammatory drugs or regional anaesthesia cannot be administered or is insufficient. In some cases it may be wise to titrate short acting opioid variants until pain sensation is sufficiently diminished. The patient needs to be observed closely, preferably in an intensive care unit.w6
Ostermeier et al state that patients with obstructive sleep apnoea are at increased risk of developing respiratory problems postoperatively in the absence of pain. Pain would prevent the rebound of rapid eye movement sleep and diminish stage 3 and stage 4 sleep, which also predisposes to collapse of the upper airway, around the third day postoperatively.19 It is postulated that the number of possible breathing depressions would thus decline.18 Use of nasal continuous positive airway pressure preoperatively and directly postoperatively reduces the risk of developing respiratory depressions and is advised.w2
Obstruction of the upper airway
Surgery of the upper airway—especially uvulopalatopharyngoplasty and (adeno)tonsillectomy—causes tissue damage and produces oedema and occasionally (considerable) haematomas. These changes can instigate or increase narrowing of the upper airway and even lead temporarily to severe obstructive sleep apnoea, particularly when opioids and sedating drugs are administered as well.20 21 Mortality after reconstruction of the soft palate (palatoschisis), due to obstruction of the upper airway, has been reported.22 23 Patients with severe obstructive sleep apnoea will need prolonged tracheal intubation or tracheotomy. Oxygen should be administered only with caution, because the ventilation process may be dependent on its “hypoxic” drive. Oxygen cannot prevent apnoea but may reduce its duration and the impact of the resulting oxygen desaturation.1 24
Nasal obstruction also has a role in the natural history of obstructive sleep apnoea, but its impact as a contributing factor remains unclear. Nasal surgery alone seems to cure only 16% of patients with obstructive sleep apnoea and nasal obstruction.25 Decreased nasal passage may not be the major contributor to obstructive sleep apnoea, but nasal or sinus surgery with use of packs does constitute an extra risk. Observation in a medium or high care unit as long as the packs are in place is advisable, and in the case of severe obstructive sleep apnoea full face continuous positive airway pressure is needed to prevent dangerous apnoeas. The effectiveness of a therapeutic alternative—a ventilation channel inside the nasal pack—is often very disappointing. Use of mattress sutures alone, without packs, could be of great value.
Additional educational resources
Review articles
Loadsman JA, Hillman DR. Anaesthesia and sleep apnoea. Br J Anaesth 2001;86: 254-66
American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Practice guidelines for management of the difficult airway: an updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Anesthesiology 2003;98: 1269-77
Esclamado RM, Glenn MG, McCulloch TM, Cummings CW. Perioperative complications and risk factors in the surgical treatment of obstructive sleep apnea syndrome. Laryngoscope 1989;99: 1125-9
Clinical papers
Ostermeier AM, Roizen MF, Hautkappe M, Klock PA, Klafta JM. Three sudden postoperative respiratory arrests associated with epidural opioids in patients with sleep apnea. Anesth Analg 1997;85: 452-60
Chung F, Imarengiaye C. Management of sleep apnea in adults. Can J Anaesth 2002;49: R1-6
Useful websites
Anesthesiology (http://www.anesthesiology.org)—provides information about practice guidelines for management of the difficult airway
American Sleep Apnea Association (www.sleepapnea.org/evaluated.html)—for more information about obstructive sleep apnoea and anaesthesia
Gupta et al found a twofold increased risk of developing complications in patients with obstructive sleep apnoea who had knee or hip surgery compared with patients without obstructive sleep apnoea after the same operation.7 Use of nasal continuous airway pressure preoperatively and postoperatively greatly reduced this complication risk.w2
Conclusion
Patients with obstructive sleep apnoea are at high risk of developing postoperative complications when having surgery or other invasive interventions under general anaesthesia. This holds true for both surgery related to obstructive sleep apnoea and unrelated surgery. Surgeons of all specialties, as well as anaesthetists, should be aware of the fact that undiagnosed obstructive sleep apnoea is common. They should be alert to patients who are at risk of having obstructive sleep apnoea and should be aware of the potential preoperative and postoperative complications in such patients having surgery. In the case of a medical history suggestive of obstructive sleep apnoea, particularly in obese patients with a short bulky neck and a large tongue, full night polysomnography should ideally be done before surgery takes place. Options that should be considered include alternative methods of pain relief, use of nasal continuous positive airway pressure before and after surgery, and surveillance in an intensive care unit, especially after nasal surgery in which packs are used. An elaborated algorithm for management of difficult airways should be established.
Information for patients
Respironics (http://www.sleepapnea.com)—gives useful information about symptoms of obstructive sleep apnoea
Anesthesia and the apnea patient (www.healthyresources.com/sleep/apnea/contrib/anesthes.html)—explains some important considerations for patients with obstructive sleep apnoea having surgical or medical procedures involving anaesthesia
eMedicine (www.emedicine.com/ent/topic370.htm)—an article about snoring, obstructive sleep apnoea, and surgery
Footnotes
 Extra references are on bmj.com
Extra references are on bmj.com-
Contributors NdV and CdH were responsible for the idea and design of the study. CdH had overall responsibility for the data collection and drafted the manuscript. All authors contributed to interpretation of the data and revising the paper.
-
Funding None.
-
Competing interests None declared.