



GPs Meet Rare Lung Disorders Task Force factsheet: α-1 antitrypsin deficiency
- Bruno Balbi⇑
- Divisione di Pneumologia, Riabilitativa, Fondazione Salvatore, Maugeri, I.R.C.C.S., Via Revislate 13, 28010 Veruno, Novara, Italy
- Bruno Balbi, Divisione di Pneumologia, Riabilitativa, Fondazione Salvatore, Maugeri, I.R.C.C.S., Via Revislate 13, 28010 Veruno, Novara, Italy. E-mail: bruno.balbi{at}fsm.it
Abstract
Definition α-1 antitrypsin deficiency (AATD) is a genetic disorder that manifests as pulmonary emphysema, liver cirrhosis and, rarely, as the skin disease panniculitis, or as vasculitis and is characterised by low serum levels of AAT, the main protease inhibitor in human serum.
Key messages
-
Think about AATD if your patient had emphysema at younger age.
-
Assess the levels of blood AAT to ascertain the diagnosis by the finding of reduced levels.
-
Refer the patient to a Department with experience in lung/liver manifestations of AATD.
-
Follow the patient longitudinally in collaboration with the reference center. Issues to consider are replacement therapy (if needed or available) and clinical evolution toward respiratory or liver failure.
Prevalence
The prevalence in the general population in Europe is approximately 1 in 2000–5000.
Clinical manifestations
The main symptom is dyspnoea, initially only on exertion and then also at rest. Cough and sputum, recurrent wheezing and variably frequent and severe exacerbations of symptoms may also be complaints of the patients. For patients with liver disease, jaundice or elevated liver enzymes can be the only manifestations in neonatal, paediatric or adult age. Early onset emphysema predominantly bibasilar (fig. 1) chronic obstructive pulmonary disease (COPD) (fig. 2), asthma and bronchiectasis (fig. 1) or a combination of these can be the respiratory clinical manifestations of AATD. Smoking is a co-factor determining lung disorders. It is estimated that approximately 1–3% of patients with COPD may have AATD. A disproportion between the history of smoking and the severity of the disease and/or the relatively young age of the patient should be regarded as suspicious of an underlying AATD. Never smokers can also manifest lung disease and it is estimated that AATD patients represent an important proportion of never smokers with COPD. Chronic hepatic disorder, cirrhosis and hepatocarcinoma are associated with AATD. Asymptomatic individuals with normal liver and lung function can be detected in family screenings for AATD.

Characteristic chest computed tomography showing bibasilar bronchiectasis and chest radiograph showing bibasilar emphysema.

Example of a spirometric curve showing severe airflow limitation. The patient, a 58-year-old male with a history of 50 pack-years, had reduced forced expiratory volumes (post-bronchodilator forced expiratory volume at 1 second <30% predicted) and thus was in GOLD Stage IV (very severe COPD). He also had chronic respiratory failure (partial pressure of oxygen in arterial blood at rest on room air of 49 mmHg) requiring longterm oxygen therapy and a reduced (52% predicted) diffusion for CO.
Conditions in which to consider AATD
-
Early onset emphysema (<45 years)
-
Emphysema without a recognised risk factor (smoking, occupational dust exposure, etc.)
-
Emphysema with prominent basilar hyperlucencies
-
Otherwise unexplained liver disease
-
Necrotising panniculitis
-
Anti-proteinase 3-postive vasculitis (c-ANCA positive): antineutrophil cytoplasmic antibody-positive vasculitis
-
Family history of any of the following: emphysema, bronchiectasis, liver disease or panniculitis
-
Bronchiectasis without evident aetiology
Other more extensive recommendations previously issued by WHO proposed the determination of AAT levels in all asthma and COPD patients.
Modified from American Thoracic Society & European Respiratory Society Guidelines on AATD, Am J Respir Crit Care Med 2003; 168: 818–900.
Diagnosis
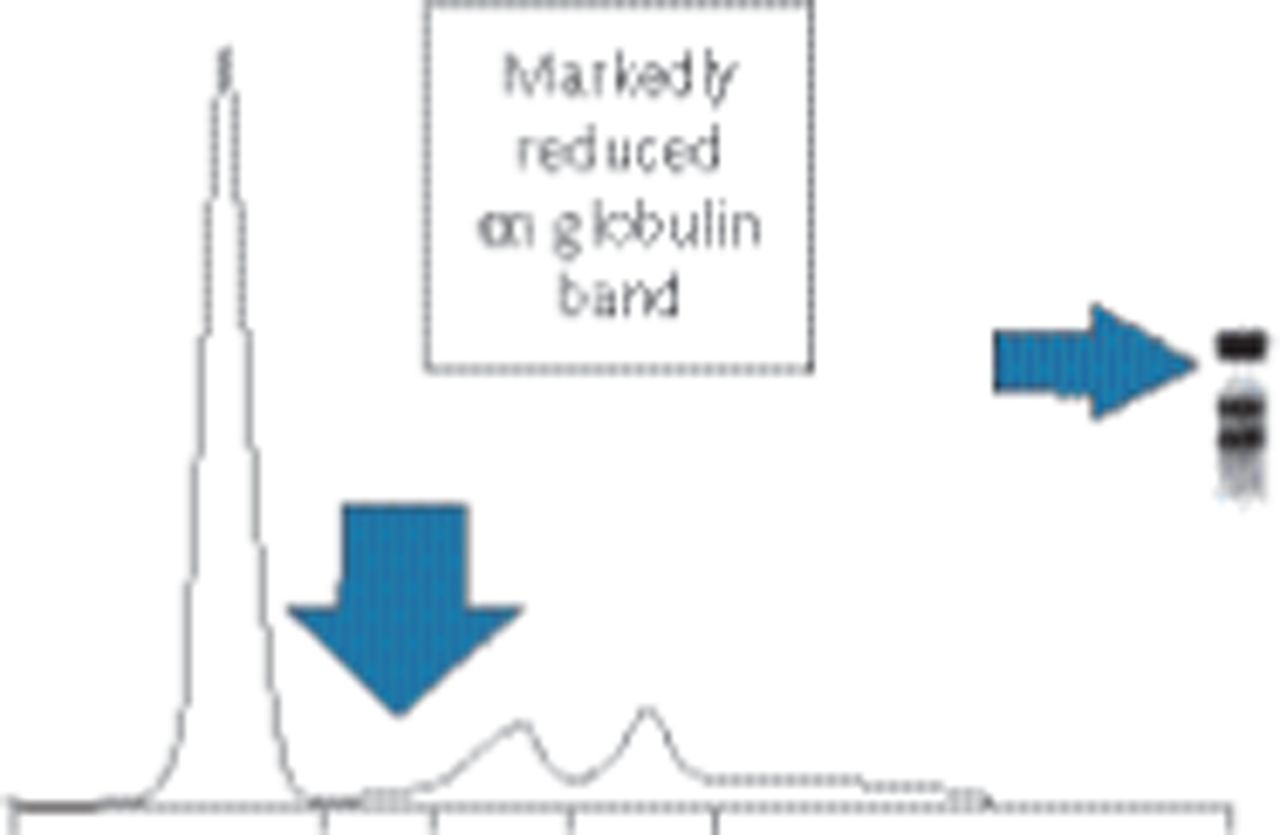
The main problem with diagnosis is the awareness that AATD can predispose to lung or hepatic diseases. Diagnosis is made by the demonstration of reduced blood levels of AAT. Reduced or absent α-1 globulin peak on serum protein electrophoresis can be an indication to determine the levels of blood AAT, as AAT comprises most of α-1 globulins (fig. 3).

{kind=link}
{kind=link}
{kind=link}
Serum protein electrophoresis of the patient in figure 2 showing markedly reduced α-1 globulin band. As most of α-1 globulins are formed by AAT, such a finding is most probably the sign of an underlying AATD, that can be ascertained by the determination of peripheral blood AAT levels, usually by nephelometry. This determination should be performed while the subject has no acute inflammatory reaction ongoing, as this can falsely increase the levels of AAT; alternatively C-reactive protein as a marker of an ongoing inflammatory condition can be co-determined to rule out falsely increased AAT levels. Reduced AAT levels associated with lung and/or liver diseases can be found in homozygous (e.g. ZZ) or double heterozygous (e.g. ZRare) patients. Intermediate levels can be found in heterozygous (e.g. MZ) individuals. The patient had 51 mg·dL−1 of serum AAT (reference values 90–200) and his genotype was ZZ.
Referral
A detailed assessment and staging of lung and/or liver disease should follow diagnosis. Depending on the National or local health system organisation, this can be performed in a reference centre specialised in AATD, as identified from its record in clinical and scientific expertise. The genotyping of the different deficient alleles (Z, S or rare alleles) is needed to better categorise patients and their clinical characteristics.
Treatment and follow-up
Treatment for COPD patients with AATD is similar to the one in non-AATD-related COPD (including inhaled bronchodilators and steroids, immunisations, rehabilitation, oxygen and lung surgery) a part from AAT replacement therapy. Replacement therapy consists of a life-long i.v. weekly infusion of exogenous purified AAT, aimed at replacing the missing AAT in the lung. Not all European countries reimburse this treatment. The main reason is because it is expensive and clinical trials, as frequent in rare disorders, were not able to undoubtedly prove its ability to slow the accelerated loss of lung function seen in these patients. In liver disease, apart from usual care supportive treatment, liver transplantation is an option, as it for lung transplantation for end-stage patients. Patients can get in touch with National Patients' Associations for more information and support.
- ©ERS 2014
Breathe articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.